

Chairman Jordan, Ranking Member Nadler, Chairman Biggs, Ranking Member Jackson Lee, and Members of the Subcommittee:
Thank you for holding this hearing today on the subject of fentanyl and fentanyl-related substances (FRS).
My background is in conservative politics. Prior to joining the bipartisan nonprofit Due Process Institute in March 2021, I served as the vice president of legislative affairs for FreedomWorks, a grassroots conservative advocacy organization. During the more than six years I was at FreedomWorks, I helped advance the First Step Act and the Fair Chance Act, both of which became law, and was involved in the introduction of, and worked on, several other pieces of criminal justice reform and second-chance legislation.
The hearing today is an important one. The problem of addiction is certainly not new to the United States. More than 50 years ago, in 1971, President Nixon declared, “[P]ublic enemy number one in the United States is drug abuse.” And since then, Congress has spent more than $1 trillion fighting an unwinnable war against the abuse of controlled substances.
Recent data provided by the National Center for Drug Abuse Statistics show that 21.4 percent of Americans aged 12 and older have used illicit drugs or misused prescription drugs in the past year. Tragically, 25.4 percent of illicit drug users suffer from substance abuse disorder. In response to sobering statistics like these, between FY 2014 and FY 2022, Congress authorized more than $293 billion for National Drug Control Program agencies, 51.5 percent of which has gone to illicit drug supply reduction, including law enforcement and other interdiction measures.
But the staggering financial cost is only one impact our war on crime has had on our nation. Congress has enacted harsh mandatory minimum prison sentences for drug offenses as well as a number of sentencing enhancements, resulting in a federal prison population in which people incarcerated for drug-related offenses are the second highest category. Incarceration also has a devastating long-term impact on families and communities, as the 2014 study, The Growth of Incarceration in the United States: Exploring Causes and Consequences, explains:
“The policies that produced very high rates of incarceration grew out of a historical period of rapid change and social conflict. By greatly expanding the use of penal confinement, the policies charted a new direction for the American criminal justice system. No other Western democracy went so far down this path. Through the 1990s and 2000s, crime rates fell significantly, but the evidence indicates it is unlikely that the rise in incarceration rates played a powerful role in this trend. Against weak evidence for large benefits, there is also the chance of significant social costs for individuals who are incarcerated, their families, and communities. The strong correlation of incarceration with unemployment, poverty, family disruption, poor health and drug addiction is very clear. Causality is harder to disentangle, but experiments and statistical adjustment point to the real possibility of negative social effects. These correlations and negative effects are concentrated almost entirely in poor, especially poor minority, communities. For policy and public life, the size of the effects of incarceration may be less important than the overwhelming evidence of the correlation between very high levels of incarceration, race, poverty, and the myriad of accompanying social problems.”
Although this hearing addresses FRS, actions taken by Congress to address concerns about other controlled substances, such as methamphetamine, show us that harsher penalties simply do not solve the problem. For example, Congress included the Methamphetamine Trafficking Penalty Enhancement Act in the Omnibus Consolidated and Emergency Supplemental Appropriations Act for FY 1999. Prior to its passage, 10 grams of methamphetamine carried a five-year mandatory minimum sentence and 100 grams carried a ten-year sentence. The Methamphetamine Trafficking Penalty Enhancement Act reduced the quantities of drugs necessary to trigger the five- and ten-year mandatory minimum sentences by half, to 5 grams for the five-year sentence and 50 grams for the ten-year sentence. But this harsher approach did not have its intended effect. When the law was being passed, methamphetamine was the primary drug choice for only 11.4 percent of individuals sentenced for drug trafficking. That figure rose to 48.3 percent by FY 2021.
Unfortunately, demand for methamphetamine has grown despite increased incarceral risk. In Kansas, the cost of an ounce of methamphetamine dropped from $1,075 in 2014 to $500 in 2021 because of the readily available supply of the substance. The director of the Kansas Bureau of Investigation, Kirk Thompson, explained, “No matter what the drug is, law enforcement can’t solve that problem alone. The demand by our citizens, the demand from people here for the illegal drugs, drives that supply chain.” He added, “Until we can all work together and address addiction . . . what we are seeing is significantly higher levels of drug abuse. [And] drug abuse and drug use fuel so much of the crime that we see in this state.” And what is happening in Kansas is happening everywhere else.
There is no denying that the opioid crisis has taken a significant toll on our country. More than 107,000 people died from drug overdoses in 2021, nearly 70,000 of them as a result of synthetic opioid-related overdoses. The incalculable impact of this crisis highlights the need for Congress to invest its attention in adopting workable solutions that reduce the demand for controlled substances through harm reduction strategies and treatment for abuse and addiction.
I note that Congress has already taken certain healthcare-centered steps in recent years to address the opioid crisis through the Comprehensive Addiction and Recovery Act, the 21st Century Cures Act, and the SUPPORT for Patients and Communities Act. Together, these three laws authorized $8.1 billion between FY 2017 and FY 2023 to reduce the demand for opioids. The SUPPORT for Patients and Communities Act also increased mandatory spending by $1.9 billion over the same period to help address the crisis. More resources like these are still needed from Congress to help states and communities address challenges caused by opioids, fentanyl, and FRS, but other steps that have been taken administratively—and since extended by Congress—are exactly the wrong way to address this crisis.
Permanent Class-Wide Scheduling of FRS Is the Wrong Policy Prescription
In February 2018, the Drug Enforcement Agency (DEA) used its statutory authority to temporarily schedule FRS, on a class-wide scale, under Schedule I of the Controlled Substances Act. Although the temporary scheduling of any substance expires after two years, Congress has routinely extended the class-wide scheduling of FRS, beginning in January 2020, and most recently in December 2022. The current extension expires at the end of calendar year 2024.
The approach that the DEA and Congress have taken thus far, as well as recent efforts in Congress to make the class-wide scheduling of FRS permanent are problematic.
For a substance to be placed on Schedule I, it must not have an acceptable medical use and must have a high potential for abuse. But legitimate research of Schedule 1 substances, which could discover beneficial medical uses, has proven difficult. An April 2021 report published by the Government Accountability Office highlighted the scope of the problem that researchers face when seeking approval from the DEA and the Food and Drug Administration (FDA) to research FRS:
“While DEA has approved all 28 researchers who applied to study fentanyl-related substances since 2018, representatives from research organizations we interviewed and articles we reviewed indicated that a Schedule I designation can hinder research on such substances. For example, according to federal officials and representatives from three research organizations, the process for obtaining approval from DEA to conduct research on Schedule I substances can be time consuming and confusing. This process includes the need to obtain approval from states and institutions (such as universities), as well as the time for DEA and FDA to conduct their reviews. In addition, according to representatives from five research organizations we met with and articles we reviewed, the time and resources it takes to meet these requirements may result in less research being conducted on both what makes these substances dangerous as well their possible use in medical treatments. Officials at NIH and some research organizations we spoke with stated that it can take more than a year to gain all of the necessary approvals to conduct research on Schedule I substances in general.”
Although FRS have been placed under Schedule I, fentanyl itself has been placed on Schedule II because it has an accepted medical use despite its high potential for abuse. However, a representative from the FDA testified before the Energy and Commerce Subcommittee on Health in December 2021 that at least one FRS may have a positive medical use in the fentanyl crisis. The FDA representative stated, “[W]e have looked at a group of somewhere over 25 FRSes, and we have studied their pharmacology. Among that group, there are members of that class, and one in particular, that has no activity to turn on the opioid receptor that we worry about here. In fact, it looks like an antagonist. It looks like it would be a blocker of the mu opioid receptor in the way Naloxone is a blocker of the mu opioid receptor . . . . This would be a substance that would have some potential for being a treatment for fentanyl.”
In the same December 2021 hearing, there was a particular focus from some Members on the high number (4,800) of potential FRS. However, this figure is hypothetical. A representative from the Office of National Drug Control Policy (ONDCP), in written testimony, acknowledged that “less than one percent of the analogues capable of being synthesized from existing molecules have been seized and identified.” In the hearing, the ONDCP representative explained that Congress has classified an entire group of substances, a large portion of which do not actually exist, as being harmful or having no medical merit despite the fact that some are no “more harmful than water.”
The injustice this scientific quandary creates in our criminal law is apparent. Although a FRS may not be harmful or have any potential for abuse, individuals who are prosecuted for interacting with them will still be subject to lengthy mandatory minimum prison sentences. This was a concern expressed in a bipartisan July 2019 letter to then-Health and Human Service Secretary Alex Azar, the signatories on which included Sens. Dick Durbin (D-IL) and Mike Lee (R-UT). The letter explained, “[I]f the class-wide scheduling is enacted, a person found in possession of one of these substances—even one with no demonstrated negative psychoactive effects—could now be subject to harsh criminal penalties established by the Controlled Substances Act and the United States Sentencing Commission Guidelines. Even more alarming, that person would have no opportunity to challenge her charge or sentence even if she is able to prove that the substance in question was completely benign.”
Unfortunately, of the legislative proposals introduced in the 118th Congress to make class-wide scheduling of FRS permanent, few offer an off-ramp to remove or reschedule an FRS that is proven to have a medical use or is inert. Should Congress move forward with a legislative solution on FRS, exceptions for substances with a medical benefit or which are otherwise harmless must be provided.
Since the DEA temporarily scheduled FRS class-wide in February 2018, and Congress subsequently extended that order, more than 170,000 people died in fentanyl-related overdose incidents between 2018 and 2021. Relevant to the subject of this hearing, I note that, even with the restrictions on border crossings in response to the COVID-19 pandemic, the number of fentanyl-related overdoses continued to climb in 2020 and 2021. Politicians have often used the death toll to highlight the need for harsher criminal laws. Unfortunately, those politicians are unwilling to recognize that our previous attempts to imprison our way out of the crisis have not worked. That mentality has to change. After more than a half a century of unsuccessful attempts to deter illicit drug usage, we have to recognize that demand for drugs grows ever higher and that addiction is a serious national health issue. A holistic approach to these challenges is necessary and include making investments in harm reduction strategies, such as increased access to naloxone and testing strips, and treatment for abuse and addiction.
Fentanyl and Our Southern Border
At the onset of the opioid epidemic, China served as the primary source of illicit fentanyl. And while efforts by the previous Administration successfully stemmed the direct supply of fentanyl from China into the U.S. unfortunately, the flow of precursors (chemicals used to manufacture illicit drugs) from China to transnational drug cartels in third countries, continues. Those substances are ultimately trafficked in large quantities into the United States.
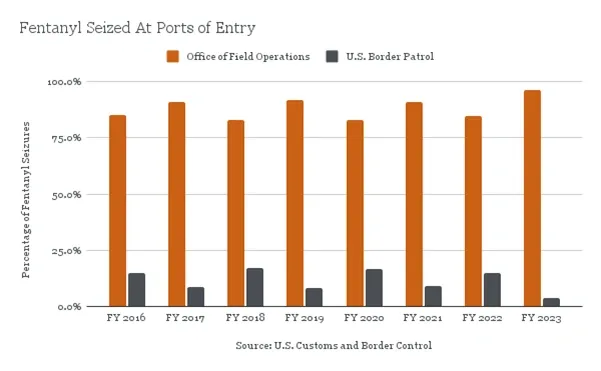
Although it is accurate to say that the majority of seized fentanyl is discovered at our Southwestern border, that is only part of the picture and the way this information is presented to the public fails to recognize an important detail: it is American citizens—not undocumented individuals—who are responsible for the vast majority of the drug trafficking via our Southern border. This surprising truth arises from enforcement data from U.S. Customs and Border Protection (CBP). CPB’s fentanyl seizures are executed by two different bodies within CBP:
“The first, the Office of Field Operations (OFO), enforces immigration and customs laws at ports of entry—points where someone may lawfully enter the United States. The second is U.S. Border Patrol, which intercepts undocumented individuals and illegally imported goods between those ports of entry.”
“The vast majority of fentanyl seized in recent years has been obtained by the OFO, not Border Patrol.”
Specifically, in FY 2022, 85 percent of fentanyl was seized by the Office of Field Operations while only 15 percent was seized by U.S. Border Patrol. Thus far in FY 2023, 96.2 percent of fentanyl was seized by the Office of Field Operations at ports of entry or check points.
In addition, the Government Accountability Office analyzed drug seizure events involving U.S. Border Control and found that “91 percent (16,315 events) involved only U.S. citizens and 4 percent (761 events) involved one or more potentially removable people.” Politicians are failing to acknowledge this kind of data when speaking about border security and are failing to recognize that it is our own citizens—not undocumented persons—who are responsible for the vast majority of the drug trafficking via our Southern border.
Conclusion
Congress does need to act, but it should not do so irresponsibly by making the class-wide scheduling of FRS permanent without exceptions for FRS with a medical benefit or those that are inert or harmless. We also should end the incarceration of people for possession of substances that are harmless or have medical benefits. Congress must also ease the ability for researchers to study FRS to determine what, if any, beneficial medical use they might have or to determine if they are harmless. Finally, lawmakers should take heed of the drug policy failures of the last several decades and treat this crisis as the public health issue that it is, which would mean focusing attention and funding more on addiction treatment and harm reduction strategies than on prosecutions and incarceration.
My hope is that the distinguished Members of this Subcommittee will use this hearing as an opportunity to search for and achieve bipartisan consensus on this critical public health issue facing the United States.
Thank you for your attention to this important issue.
Sincerely,
Jason Pye
Director, Rule of Law Initiatives
Due Process Institute
700 Pennsylvania Avenue SE, Suite 560
Washington, DC 20003
Jason@iDueProcess.org
(202) 558-6686